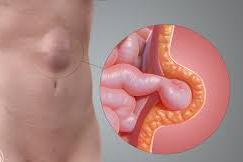
What is a ventral hernia?
A ventral hernia usually arises in the abdominal wall where a previous surgical incision was made. In this area the abdominal muscles have weakened; this results in a bulge or a tear. In the same way that an inner tube pushes through a damaged tire, the inner lining of the abdomen pushes through the weakened area of the abdominal wall to form a balloon-like sac. This can allow a loop of intestines or other abdominal contents to push into the sac. If the abdominal contents get stuck within the sac, they can become trapped or “incarcerated.” This could lead to potentially serious problems that might require emergency surgery.
Other sites that ventral hernias can develop are the belly button (umbilicus) or in the area between the breast bone and the belly button (epigastric). A hernia does not get better over time, nor will it go away by itself.
How do I know if know if I have a hernia?
A hernia is usually recognized as a bulge under your skin. Occasionally it causes no discomfort at all, but you may feel pain when you lift heavy objects, cough, strain during urination or bowel movements or with prolonged standing or sitting.
The discomfort may be sharp or a dull ache that gets worse towards the end of the day. Any continuous or severe discomfort, redness, nausea or vomiting associated with the bulge are signs that the hernia may be entrapped or strangulated. These symptoms are cause for concern and immediate contact of your physician or surgeon is recommended.
What causes a ventral hernia?
An incision in your abdominal wall will always be an area of potential weakness. Hernias can develop at these sites due to heavy straining, aging, injury or following an infection at that site following surgery. They can occur immediately following surgery or may not become apparent for years later following the procedure.
Anyone can get a hernia at any age. They are more common as we get older. Certain activities may increase the likelihood of a hernia including persistent coughing, difficulty with bowel movements or urination, or frequent need for straining.
Laparoscopic or Keyhole repair of Ventral (incisional) hernias Ventral (incisional) hernias
Many ventral hernias are performed by the conventional “open” method. Some are performed laparoscopically.
Laparoscopic hernia repair is a technique to fix tears or openings in the abdominal wall using small incisions, laparoscopes (small telescopes inserted into the abdomen) and a mesh is used to reinforce the abdominal wall defect. It may offer a quicker return to work and normal activities with decreased pain.
What are the advantages of the laparoscopic repair?
Results may vary depending on the type of procedure and each patient’s overall condition. Common advantages may include: Less post-operative pain, Shortened hospital stay, Faster return to regular diet and quicker return to normal activity. The disadvantages are increased cost because of the cost of the Consumables (Mesh and Tackers to fix it)
Recently eTEP -RS and eTEP-TAR are newer laparoscopic techniques that is used to place large meshes in a deeper plane but separate from the intraabdominal contents. This is a specialized technique and gives equally good or better results in selected patients.
Are you a candidate for the laparoscopic repair?
Only after a thorough examination can your surgeon determine whether a laparoscopic ventral hernia repair is right for you. The procedure may not be best for some patients who have had extensive previous abdominal surgery, hernias found in unusual or difficult to approach locations, or underlying medical conditions.
How is the procedure performed?
The two methods of ventral hernia repair are:
- The traditional or ‘open’ approach is done through an incision in the abdominal wall. It may go through part or all of a previous incision, skin, and an underlying fatty layer and into the abdomen. It then requires the placement of mesh in or on the abdominal wall.
- The second approach is a laparoscopic ventral hernia repair. In this approach, a laparoscope (a tiny telescope with a television camera attached) is inserted through a cannula (a small hollow tube). The laparoscope and TV camera allow the surgeon to view the hernia from the inside. Other small incisions will be required for other small cannulas for placement of other instruments to remove any scar tissue and to insert a surgical mesh into the abdomen. This mesh is fixed under the hernia defect to the strong tissues of the abdominal wall. It is held in place with special surgical tacks and in many instances, sutures. Usually, three or four 1/4 inch to 1/2 inch incisions are necessary. The sutures, which go through the entire thickness of the abdominal wall, are placed through smaller incisions around the circumference of the mesh. This operation is usually performed under general anaesthesia.
What should II expect after surgery?
Patients are encouraged to engage in light activity while at home after surgery. The extent of activity, including lifting and other forms of physical exertion will be advised by the surgeon.
Post-operative discomfort is usually mild to moderate. Frequently, patients will require pain medication. Most patients are able to get back to their normal activities in a short period of time. These activities include showering, driving, walking up stairs, lifting, work and sexual intercourse. Occasionally, patients develop a lump or some swelling in the area where their hernia had been. Frequently this is due to fluid collecting within the previous space of the hernia. Most often this will disappear on its own with time. If not, your surgeon may aspirate this with a needle in the outpatient clinic.
What complications can occur?
Although this operation is considered safe, complications may occur as they might occur with any operation. Complications during the operation may include adverse reactions to general anaesthesia, bleeding, or injury to the intestines or other abdominal organs. If an infection occurs in the mesh, it may need to be removed or replaced.
When to contact your doctor?
If you develop any of the following at home after your discharge then you should contact the surgeon urgently. The symptoms are Persistent fever over 101 F (38.3 C), Bleeding, Increased abdominal swelling or pain, Pain that is not relieved by your medications, Persistent nausea or vomiting, Chills, Persistent cough or shortness of breath, Drainage from any incision or Redness surrounding your incisions.
|